
Impingement is one of the most commonly cited but misunderstood diagnoses of shoulder pain. Let’s examine the definition of impingement first.
If something is impinged upon it is being pinched by something else.
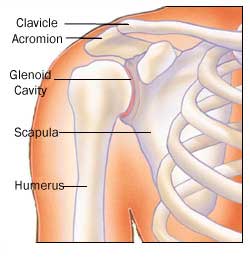
Historically, it’s been thought that when some people raise their arm above shoulder level their rotator cuff tendons pinch or impinge against bone spurs under the shoulder blade (acromion). The rotator cuff muscles enter the shoulder joint underneath the acromion so this seems to make sense.
While sometimes this is true, it is not true of all patients who are told that they have impingement.
It is now better understood that impingement has as much to do with the internal properties of the rotator cuff tendon itself as the external sources of pressure on the tendons. There is good evidence to support this.
Studies have tried to correlate the shape of the acromion process with patients’ impingement symptoms. If impingement was completely a phenomenon of the acromion pressing on the rotator cuff, it would stand to reason that patients with a more hook-shaped acromion, which would allow less space for the rotator cuff to pass, would have more pain. However, studies have never demonstrated a strong link between “impingement” symptoms and the increased hook shape of the acromion.
Regardless, the concept of acromion shape took root in the minds of surgeons and has often been used to justify surgery called acromioplasty. The concept is not entirely wrong: some patients DO have pinching of the rotator cuff by the acromion. It is just that this is an incomplete picture.
In fact, acromioplasty typically DOES eliminate impingement symptoms. Fortunately in many cases, other less invasive treatments like physical therapy also do too.
It is important to know this because many patients get the impression that it is absolutely necessary to get rid of the bone spurs on the acromion to get rid of their pain. But that is not always the case.
Nonsurgical Intervention May Provide Just As Much Relief
It’s been shown that in the long run, surgery to remove bone spurs and inflamed bursa is equally as effective in many patients as doing common physical therapy exercises.
Recent studies have also shown that patients undergoing rotator cuff surgery who have acromion bone spurs removed do just as well as patients who do not. Logic also tells us that if all impingement was due to bone spurs pressing on the rotator cuff, then the tears seen in the cuff should all start on the side that is pinched. But they don’t.
Why the misunderstanding then? It may be a case of intuition leading us astray. In other words, it makes sense in our minds that bone spurs would press on the rotator cuff and cause irritation and pain.
So when you are told that you need bone spurs removed, understand that the impingement syndrome is slightly more complex. Understand also that surgery or therapy often have equally good results for some patients. Those people who do well with surgery, often times are the ones who have failed to do well with a long course of physical therapy.
In my personal experience, I have found patients that fail a course of therapy (at least 3-6 months) will often have at least a partial thickness rotator cuff tear that will benefit from surgery. Think of the physical therapy as a test. For most people it will work. However, the only way to know whether it will work is to try it. For those in which it does NOT work or in those that have to return to function more rapidly, surgery is often a good option.